

At the start of a hospital shift, clinicians are not searching for data. They are surrounded by it. Overnight vitals, lab results, medication changes, consult notes, and operational updates are all captured across the system with precision.
The challenge is not access to information, nor the ability to interpret it. Clinicians are trained to synthesize complex inputs and make decisions under pressure. They do this every day, often with remarkable consistency.
What has changed is the scale at which they are expected to do it—and the systems through which that information must be assembled.
As patient volumes rise and cases grow more complex, the effort required to form a complete, real-time picture of patient status has increased. Information exists, but it is distributed. Signals are captured but not always connected. The system reflects activity, but not always context.
Healthcare is not running out of clinicians fast enough to explain the crisis. It is running out of system capacity to support them.

A Growing Population Meets a Static Model
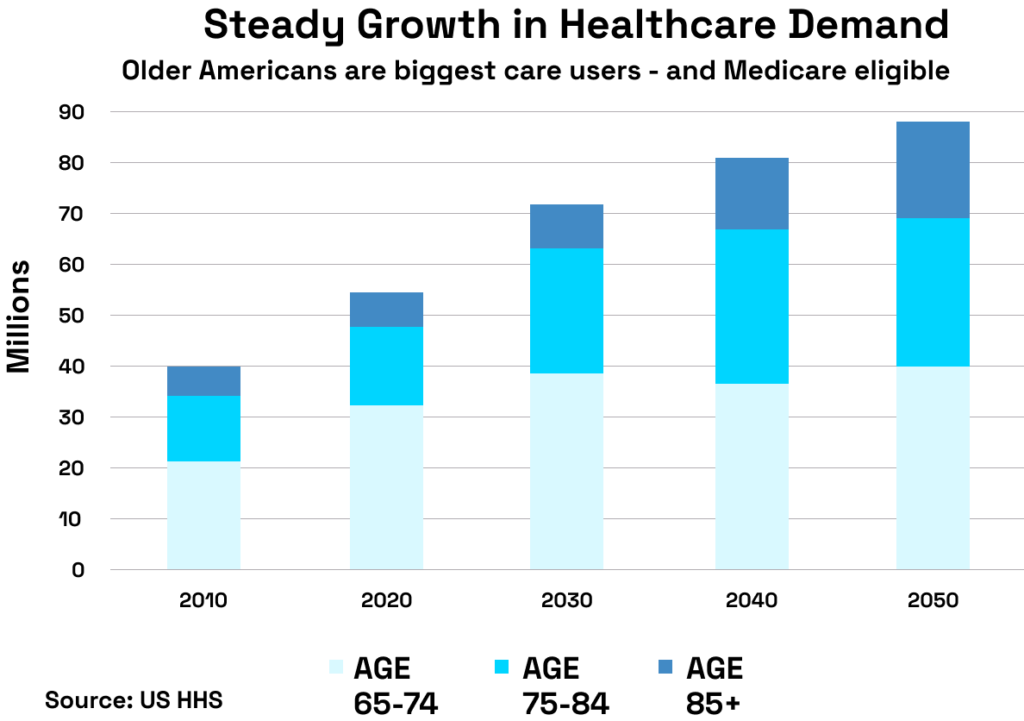
By 2030, one in five Americans will be over the age of 65. This is not simply a demographic milestone; it is a structural inflection point for healthcare delivery. Older populations require more frequent, more complex, and more coordinated care. Chronic conditions are no longer managed episodically but across extended periods, often involving multiple specialties and care settings.
At the same time, the workforce is not scaling at the same rate. Global projections estimate a shortfall of up to 18 million healthcare workers by the end of the decade, while the United States alone may face a physician deficit of up to 139,000 by 2036. These figures are well understood, and health systems have responded with urgency—expanding training pipelines, investing in retention strategies, and redesigning care teams.
Yet even as these efforts continue, the strain persists. Not because the workforce is incapable of meeting demand. But because the system in which that workforce operates was not designed to.
Fragmentation at Enterprise Scale
Large health systems have achieved significant progress in standardization. Enterprise electronic health records, centralized reporting, and shared protocols have improved consistency across care delivery. But beneath that standardization, fragmentation remains.
Clinical, operational, and real-time data are generated continuously across the enterprise, yet they are rarely unified into a single, coherent layer of insight. Monitoring systems operate alongside—but not within—clinical workflows. Operational data informs staffing and throughput but is not consistently connected to patient-level decision-making. Analytics platforms generate valuable insights, but too often outside the moment where those insights are needed.
This fragmentation does not prevent care from being delivered. It constrains how effectively that care can be delivered at scale.
Clinicians compensate for this gap through experience, training, and judgment. They assemble context across systems, prioritize under pressure, and act with precision. But as complexity increases, the reliance on human synthesis becomes the limiting factor.
No workforce, no matter how skilled, can scale against a system that fragments the information it depends on.
What the Data Makes Clear
The pressures facing health systems are not theoretical. They are measurable, persistent, and accelerating.
Across global and U.S. data, several patterns converge:
- A projected global shortage of approximately 11 million workers in critical healthcare roles by 2030, with the United States facing significant deficits across physicians, nurses, and specialty roles,
- Persistent burnout and turnover, with emotional stress identified as a leading driver of workforce attrition.
- Increasing patient acuity and demand, particularly among aging populations with complex, longitudinal care needs (see below).
- Expanding use of AI and automation, yet uneven integration across workflows, with only a portion of hospitals effectively leveraging these capabilities.
These trends point to a system under pressure. Not only because demand is rising, but because existing capacity is being consumed inefficiently.
Progress Is Real, But Not Yet Systemic
There is no shortage of innovation within healthcare systems. Across the country, organizations are demonstrating what is possible when technology, workflows, and care models are aligned.
Houston Methodist increased operating room capacity by 15% without adding staff through AI-enabled coordination. Emory Healthcare improved clinician productivity and patient experience through ambient documentation technologies. Corewell Health redirected more than 130,000 nonclinical requests away from nursing staff, saving over 25,000 hours of clinical time.
These are not marginal improvements. They are proof that capacity can be expanded without expanding headcount.
But they remain isolated.
They exist within departments, programs, and pilots—not yet as a coordinated, enterprise-wide system. Until these capabilities are connected, their impact will remain limited.
That is the gap the industry has not yet closed.
The Missing Layer: Coordination as Infrastructure
Healthcare does not lack intelligence. It lacks coordination. Not coordination as a manual effort, but as an embedded system capability—one that connects data across domains, aligns workflows in real time, and enables clinicians to act with clarity rather than reconstruction.
This cannot be solved by adding more tools. Additional layers, without integration, increase complexity and contribute to the very fatigue systems are attempting to reduce. The solution is architectural.
Platforms such as Snowflake provide the foundation for this shift by unifying clinical, operational, and real-time data into a single, governed, environment. By supporting structured, semi-structured, and streaming data at scale, Snowflake fosters greater data interoperability and removes the constraints that have historically kept data siloed and difficult to operationalize.
Within this architecture, data is no longer confined to individual systems. It becomes a shared layer of context across the enterprise—accessible in real time, consistent across teams, and capable of supporting concurrent workloads without conflict.
On top of that foundation, capabilities such as Snowflake Cortex AI enable intelligence to operate where the data lives. Rather than producing isolated outputs, AI can continuously identify patterns, prioritize risk, and surface signals within the flow of care delivery. This is what allows insight to become action.
Scaling the Workforce by Scaling the System
The healthcare workforce shortage is often framed as a supply problem: how to recruit, train, and retain more clinicians. That work will remain essential. But it will not be sufficient.
The more immediate and scalable opportunity lies in increasing the effectiveness of the workforce that already exists. When systems reduce fragmentation and enable coordinated action, capacity expands without increasing headcount.
- Clinicians spend less time assembling context and more time applying judgment.
- Operational teams respond to demand in real time rather than after the fact.
- Administrative burden is reduced, freeing capacity for direct patient care.
- Care delivery becomes more consistent across departments and settings.
This is how systems scale. Not by asking clinicians to do more.
But by removing the friction that prevents them from doing what they already do—at the level they were trained to operate.

The Decision Ahead
The healthcare workforce crisis is real, and it will intensify over the next decade. But it is not inevitable that it will overwhelm the system.
Health systems already possess much of what they need: vast amounts of data, growing investments in AI, and proven examples of operational improvement. What remains unresolved is how those elements are brought together.
Fragmentation is no longer a tolerable inefficiency. It is the defining constraint on scalability.
Platforms like Snowflake and capabilities such as Snowflake Cortex AI make it possible to resolve that constraint—not by adding complexity, but by replacing it with coordination.
The system already knows more than it can act on.
The question is whether healthcare will continue to layer solutions on top of fragmentation or finally reorganize itself to use what it already knows.
Because the future of healthcare will not be defined by how much technology it deploys. It will be defined by whether that technology allows clinicians to act—earlier, with greater clarity, and at the scale the system now demands.
If your organization is evaluating how to reduce fragmentation, scale clinical capacity, and operationalize AI across care delivery, now is the time to act.
Contact us today to explore how our industry-aligned data experts can help you design a data and AI foundation that enables real-time coordination, supports your workforce, and scales with the demands of modern healthcare.


